AUCTORES
Globalize your Research

Research | DOI: https://doi.org/10.31579/2640-1053/090
*Corresponding Author: Erlinda M. Gordon, Cancer Center of Southern California, Santa Monica CA 90403, US.
Citation: J R. Ravicz, CW. Szeto, S Reddy, S P. Chawla, M A. Morse, F L. Hall, E M. Gordon. (2021) CCNG1 oncogene: a novel biomarker for cancer therapy /gene therapy. J.Cancer Research and Cellular Therapeutics. 5(4); Doi: 10.31579/2640-1053/090
Copyright: © 2021 Erlinda M. Gordon, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 July 2021 | Accepted: 21 July 2021 | Published: 03 August 2021
Keywords: deltarex-g; human cyclin g1; cell cycle control; cancer gene therapy; oncogenic drivers; cancer stem cells; cell competence
Background: Metastatic cancer is associated with an invariably fatal outcome. However, DeltaRex-G, a tumor-targeted retrovector encoding a gene-edited dominant-negative CCNG1 inhibitor gene, has induced long term (>10 years) survival of patients with chemo-resistant metastatic pancreatic adenocarcinoma, malignant peripheral nerve sheath tumor, osteosarcoma, B-cell lymphoma, and breast carcinoma.
Objective: To evaluate the level of CCNG1 expression in tumors as a potential biomarker for CCNG1 (Cyclin G1-blocking) inhibitor therapy.
Methods: CCNG1 RNA expression levels that were previously measured as part of whole genome molecular profiling of tumors (TCGA, N=9161), adjacent “tissues” (TCGA, N=678) and GTEx normal tissues (N=7187) across 22 organ sites were analyzed. Differential expression of CCNG1 and Ki-67 in primary (N= 9161) vs metastatic (N= 393) tumors were also compared in primary (N=103) vs. metastatic (N=367) skin cancers (i.e., melanoma).
Statistical Analysis: To detect systematically differential expression of CCNG1 and Ki-67 expression between populations (e.g. tumor vs. normal), unpaired Student's t-tests were performed.
Results: Enhanced CCNG1 RNA and Cyclin G1 protein expression were noted in tumors compared to normal analogous counterparts, and CCNG1 expression correlated significantly with that of Ki-67. Moreover, CCNG1 expression tended to be higher than that of Ki-67 in metastatic vs primary tumors.
Conclusions: Taken together with the emerging Cyclin G1 / Cdk / Myc / Mdm2 / p53 Axis governing Cancer Stem Cell Competence, this supportive data indicates: (1) CCNG1 expression is frequently enhanced in tumors when compared to their normal analogous counterparts, (2) CCNG1 and Ki-67 expressions are higher in metastatic vs primary tumors, (3) CCNG1 expression is significantly correlated with that of Ki-67, and (4) CCNG1 may actually be a stronger prognostic marker of stem cell competence, chemo-refractoriness, and EMT/metastasis than Ki-67. Phase 2 studies are planned to identify patients most likely to respond favorably to CCNG1 inhibitor therapy.
Cyclins are a highly conserved family of executive regulatory proteins that govern the molecular-genetic “activation” of quiescent stem cells (i.e., Cell Competence to proliferate), as well as the definitive phases of cell cycle progression, in both normal tissue regeneration and in disease, through physical interaction with cognate cyclin-dependent proline-directed protein kinase partners (CDKs) [1,2], which phosphorylate and regulate key regulatory substrates exerting cell cycle checkpoint control. The human Cyclin G proto-oncogene (CCNG1) was originally identified/cloned, silenced-experimentally, blocked-functionally (by gene-edited dominant-negative mutation), and characterized physiologically in the crucible of clinical oncology: thereby defining “The pivotal Cyclin G1 / Cdk / Myc / Mdm2 / p53 Axis” as a prospective Unifying Theme in oncology [3,4]—identifying Cyclin G1 expression profile as a frequent feature and key oncogenic driver of cancer stem cell survival [5], c-Myc oncogenicity [6], loss of DNA fidelity [7], cancer development [8], progression [9], epithelial-to-mesenchymal transition (EMT) [9], refractoriness to chemotherapies [10], and the troublesome immune anergy [11] of advanced metastatic cancers.
The CCNG1 oncogene-a non-canonical cyclin exhibiting molecular aspects of both transcriptional regulation and cell cycle control [1,2] operates at the “first and rate-limiting step” in the animal cell cycle: that is, stem cell Competence (G0 to G1 boundary), where Cyclin G1/CDK activity phosphorylates and stabilizes the c-Myc oncogene/transcription factor [12-14], contributing to cancer progression and metastatic behavior [3-6]; while the physical association of Cyclin G1 with the Mdm2 oncogene, a ubiquitin ligase, is a negative regulator of the TP53 (p53) tumor suppressor: a guardian of DNA fidelity [7], which is commonly lost with cancer progression. As such, CCNG1 has been clinically determined to be a strategic target for cancer gene therapy.
DeltaRex-G—previously developed clinically as Rexin-G [15-19]—is a tumor-targeted amphotropic MLV-based retroviral vector: (i) displaying a collagenous Pathotropic Signature (SIG)-binding/targeting peptide on its gene-edited gp70 envelope protein [20,21], and (ii) encoding a gene-edited dominant-negative expression construct of the CCNG1 oncogene (dnG1)—the enforced expression of dnG1 blocks Cyclin G1-dependent cell survival function(s) and enforces apoptosis in a broad spectrum of cancer cells in vitro, in animal models, and clinically in advanced metastatic cancers [3,4] where notable safety, efficacy and long-term survival have been achieved (> 12 years) with repeated infusions of DeltaRex-G [22-24]. When administered intravenously, the tumor-targeted nanoparticles (~100 nm) actively seek-out and accumulate-in the tumor microenvironment (TME), binding with high-affinity to abnormal (anaplastic) SIG proteins exposed biochemically during tumor invasion, tumor angiogenesis, and/or reactive stroma formation [25]. Treatment with DeltaRex-G has demonstrated objective clinical benefits and prolonged survival in metastatic, chemotherapy-resistant pancreatic ductal adenocarcinoma, osteosarcoma, sporadic malignant peripheral nerve sheath tumor (sMPNST), and both hormone receptor positive and triple negative ductal carcinoma of breast [3,4, 22-24]. In light of the pivotal roles and survival function of Cyclin G1 in cancer stem cell biology [5-11], the observed clinical efficacy of DeltaRex-G, including long-term survival benefits achieved in advanced, metastatic, chemo-resistant cancers, suggests that DeltaRex-G may indeed be most efficacious and comparatively advantageous in advanced metastatic tumors that overexpress the pivotal and commanding CCNG1 oncogene. Here, the aims of this investigation are to report augmented CCNG1 oncogene expression in many solid tumors and provide the rational basis for profiling Cyclin G1expression in tumors to identify patients who are likely to benefit from CCNG1 inhibitor therapy.
All archived tumor samples are de-identified tissue samples previously used for other histopathologic examination and molecular profiling studies at NantOmics Bioinformatics Department of Nant and at the Cancer Center of Southern California/Sarcoma Oncology Research Center. Written consent was obtained from patients as part of histopathologic examination and molecular profiling of archived tumors as standard of care.
The Genotype-Tissue [removed]GTEx) project is an ongoing effort to build a comprehensive public resource to study tissue-specific gene expression and regulation. Samples were collected from 54 non-diseased tissue sites across nearly 1000 individuals, primarily for molecular assays including WGS, WES, and RNA-Seq. Remaining samples are available from the GTExBio bank. The GTEx Portal provides open access to data including gene expression, QTLs, and histology images.
CCNG1 RNA Sequence Analysis
Previously obtained whole-transcriptome expression levels across 22 commensurate organ sites within three different settings: tumor tissues (The Cancer Genome Atlas [TCGA], n=9161), tumor-adjacent tissues (TCGA, n=678) and normal tissues (Genotype-Tissue Expression Portal [GTEx], n=7187) were analyzed for CCNG1 expression.
Qualification of IHC assay for Cyclin G1 expression
An anti-cyclin G1 IgG1 kappa light chain murine monoclonal antibody (Santa Cruz Biotechnology, Santa Cruz, CA, cat# sc-8016), coupled with MACH4 anti-mouse secondary antibody (BioCare Medical, Pacheco, CA) were used for immunohistochemical (IHC) analysis. The mouse monoclonal antibody was optimized on cell line tissue microarray and normal tissue microarray samples sectioned at approximately 4 μm and adhered to positively charged glass. Multiple antigen retrieval methods and a series of titrations of the cyclin G1 antibody were performed using the tissue microarray slides to determine the optimal antigen retrieval method and antibody concentration. Once the antibody concentration was chosen, accuracy, specificity, sensitivity, and the range of staining intensity was assessed using de-identified samples of hepatocellular carcinoma and breast carcinoma samples as positive controls, and normal tissues as negative controls. Additionally, three neoplastic tissues representing various degrees of cyclin G1 expression were chosen for an assessment of reproducibility and precision. Then, IHC analysis was performed on 27 de-identified formalin-fixed, deparaffinized samples, representing 13 types of cancer and 4 types of normal tissue. The optimized method is as follows: First, the samples were deparaffinized and rehydrated, and endogenous peroxidase activity was blocked. Then, antigen retrieval was performed in a decloaking chamber with Tris-EDTA for 20 minutes at 95° C. The anti-cyclin G1 antibody was applied at a dilution of 1:2000, and incubated for 30 minutes at room temperature, followed by application of the MACH4 mouse secondary antibody for 15 minutes at room temperature. A MACH4 HRP Polymer (BioCare Medical, Pacheco, CA) was then applied as the detection system, and incubated for 30 minutes at room temperature. The resulting product was incubated in chromogen DAB-beta (BioCare Medical, Pacheco, CA) for 10 minutes at room temperature, and was then counterstained with hematoxylin, dehydrated, cleared in xylene, and finally a coverslip was applied. The samples were then analyzed by a board-certified pathologist who scored the staining intensities of the samples on a scale of 0 to 3+.
Reproducibility was tested in several ways: (1) intra-run reproducibility, with identical slides run in triplicate in one run on one day; (2) inter-run reproducibility with identical slides tested on three separate runs in three separate days; (3) inter-tech reproducibility, with identical slides run by two different technologists in two separate runs; and (4) inter-instrument reproducibility with identical slides run by the same technologist on two different instruments. Concordance factors were calculated based on the pathologist’s scoring of the reproducibility slides. As an indirect confirmation of cyclin G1 assay specificity, additional IHC experiments were performed to compare expression of cyclin G1 to that of cellular proliferation marker Ki-67. Intra-run, inter-run, inter-tech, and inter-instrument reliability were all deemed as acceptable and CCNG1 expression observed by IHC was in line with that predicted in the literature.
To generate statistically comparable expression profiles for each sample, transcripts-per-million (TPM) values were generated using RSEM [26] scaled using only protein-coding transcripts, then converted to (approximately) Gaussian distributions by log2 transformation (i.e. log2[TPM+1]).
To detect systematically differential expression of CCNG1 and Ki-67 expression between populations (e.g. tumor vs. normal), unpaired Student's t-tests were performed. t-tests were employed rather than non-parametric tests (e.g Wilcoxon test) as across tissues CCNG1 and Ki-67 both displayed normal distributions (despite being skewed in some organ subsets) and non-parametric tests may be underpowered with low sample counts such as those provided in TCGA normal tissues. We evaluated cohort-level differential expression of CCNG1 and Ki-67 in primary (n=9161) vs metastatic (n=393) across organ sites. Seeing as TCGA sources provide ample metastatic samples from skin cancer (e.g. melanoma) cases, we also performed primary vs. metastatic analysis within skin cancer specifically (n=103 and n=367, respectively). Additionally, we observed differential expression of CCNG1 and Ki-67 between settings (primary and metastasis) within the same individuals. Matched pairs of primary and metastasic tumor samples were available for 28 patients across 12 organ sites in the TCGA cohort. Fold-change was calculated by taking the ratio of primary and metastatic log2-TPM values.
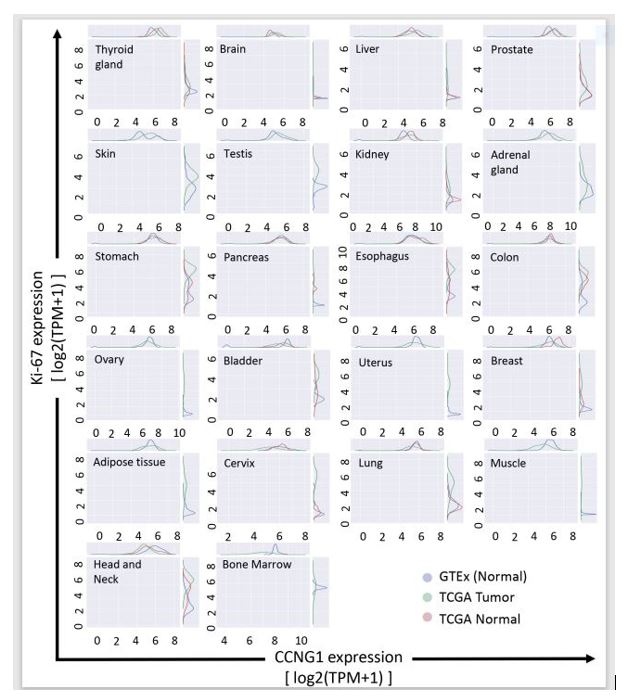
Points to Consider #1: CCNG1is overexpressed throughout the TME, including adjacent non-tumorous areas.
Figure 1 shows the differential expression of CCNG1 (x-axis) vs Ki-67 (y-axis) in tumor (green) and normal (blue and red) settings. There was no significant difference in CCNG1and Ki-67 expression across organ sites in TCGA tumor and adjacent non-tumor tissue within the TME (TCGA normal). In contrast, as shown in Table 1, CCNG1 expression was significantly enhanced in TCGA tumor compared to normal tissue obtained post-mortem from patients with no tumors (GTEX normal). This is an important observation since proliferative tumor-associated microvasculature (TAM) and tumor-associated fibroblasts (TAFs) would also show enhanced expression of CCNG1 and Ki-67 in the adjacent non-tumor tissue within the TME.

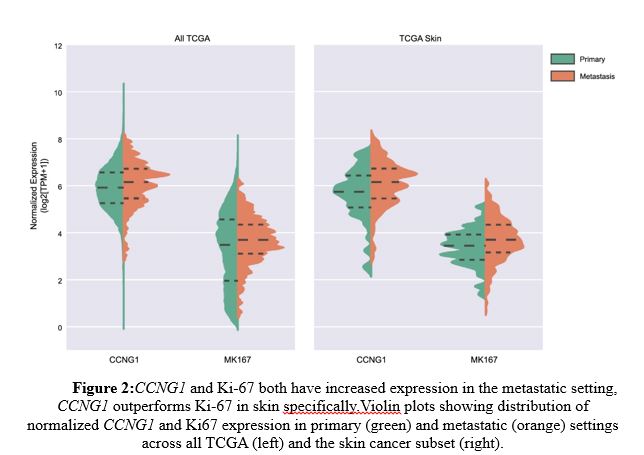
Points to Consider #2: CCNG1expression is higher than that of Ki-67 in metastatic skin cancers (e.g., melanoma, basal cell carcinoma, squamous cell carcinoma).
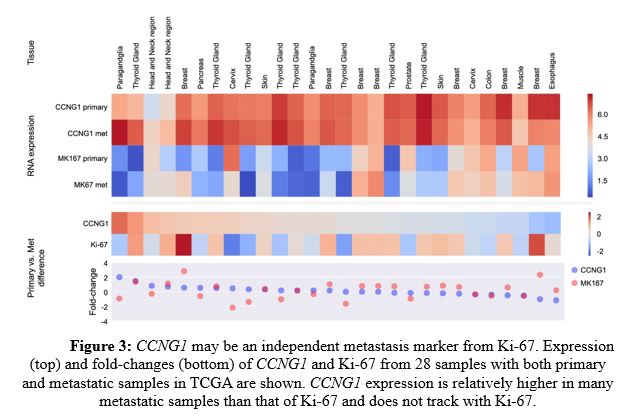
As shown in Figure 2 left panel, CCNG1 and Ki-67 both showed enhanced expression in metastatic settings (orange) compared to primary tumors (green), but CCNG1 outperformed Ki-67 specifically in metastatic skin cancer (right panel). Further, CCNG1 expression was relatively higher in many metastatic samples than that of Ki-67 and did not track with Ki-67 (Figure 3). These data indicate that CCNG1 oncogene expression may be a better indicator of metastasis than primary tumors.
Points to Consider #3: CCNG1 expression is enhanced in specific tumors by RNA sequence analysis.
As shown in Table 1, in 11 of 22 measured samples, CCNG1 RNA expression was significantly overexpressed in TCGA tumor samples compared to GTEx normal tissues, including thyroid, brain, liver, prostate, skin, testis, kidney, adrenal, stomach, pancreas and esophageal cancers.
In 4 of the 22 samples, CCNG1 RNA was under-expressed in the tumor samples, indicating that these tumors were in dormant or inactive state and as such, these tumors were not actively dividing, and may not be responsive to DeltaRex-G therapy, a retroviral based vector that integrates only in actively dividing cells [15-21].
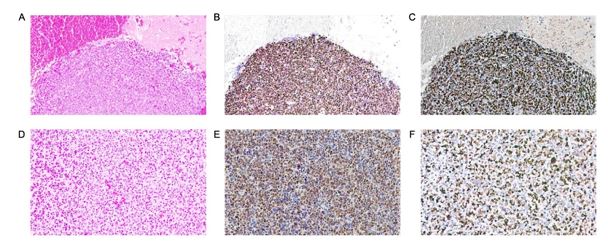
Points to Consider #4: CCNG1 nuclear protein expression is enhanced in most tumors examined by IHC.
Furthermore, IHC staining revealed significant cyclin G1 overexpression in almost all tumor samples and cancer cell lines (Table 2). For example, Figure 4 shows 80% nuclear CCNG1+ and nuclear Ki-67+ tumor cells in mesenchymal chondrosarcoma metastatic to brain.
During embryological development, the CCNG1 (Cyclin G1) oncogene product normally cooperates with the TP53 (p53) family of tumor suppressor proteins in mediating genome stability: operating at multiple cell cycle checkpoints in proliferative somatic cells [27-30]. Characterization of the CCNG1 oncogene in terms of clinical oncology (dysregulated expression, viral subversion, oncogenic interactions, and stem cell survival functions) revealed Cyclin G1 also complexes with the c-Myc and Mdm2/Hdm2 oncogenes—thus identifying the pivotal Cyclin G1 / Cdk / Myc / Mdm2 / p53 Axis of cancer stem cell competence as a strategic target for broad-spectrum cancer gene therapy [3,4] and a potentially unifying theme of cancer ontogeny (Cyclin G1-complex), EMT, and metastatic progression.
Reimer et al. [31] was among the first to describe histopathological overexpression of Cyclin G1, with subcellular localization at DNA replication foci, suggesting potential diagnostic and prognostic implications of CCNG1dysregulation in both breast and prostate cancer cells in vitro, as well as cancer cells in situ from tumor specimens, using differential display polymerase chain reaction (PCR) screening [31]. Following DNA damage, Reimer et al. showed that Cyclin G1 was triggered to cluster in a discrete nuclear pattern at DNA replication foci; demonstrating subcellular co-localizing at foci containing the replication-associated proliferating cell nuclear antigen (PCNA), which physically binds to the classic CDKN1A/ p21Waf1/CIP1-tumor suppressor [32], to regulate genomic stability, cell cycle arrest, and senescence in response to DNA damage through myriad complex physical interaction(s) with TP53 (p53)[7,33].
In 2015, Jiang et al. [34] advanced the clinical understanding of CCNG1 by investigating its molecular expression and biochemical role in governing cellular proliferation and apoptosis of epithelial ovarian cancer (EOC), where CCNG1 (Cyclin G1) was found to be upregulated in EOC tumors, compared with normal ovarian tissues. In EOC, CCNG1 expression was closely correlated with differentiation grade (P = 0.009) and malignant tumor cells in ascites (P = 0.009). The Kaplan-Meier curves showed that higher expression of CCNG1 was associated with significantly shorter survival in EOC patients, while multivariate analysis suggested CCNG1 expression is an independent prognostic factor in terms of overall survival. Combined immunofluorescence and flow cytometry analysis confirmed that silencing of CCNG1 with shRNA is lethal to EOC: promoting apoptosis of ovarian cancer cells. Taken together, Jiang et al.'s findings suggest that CCNG1 may indeed serve in the prognosis of EOC patients, as well as a prospective therapeutic target.
Likewise, a molecular histological evaluation of CCNG1 expression in colorectal neoplasia, demonstrated CCNG1 overexpression in 91% of colorectal tumors studied [35]. The Cyclin G1-positive cancer patients were evenly distributed between men and women, and between tumor locations and grading. Moreover, this comparative study noted that Cyclin G1 overexpression was a more frequent event than the commonly dysregulated CCND1/PRAD1/ Cyclin D1 proto-oncogene (found in only 42% of colorectal adenocarcinomas) [35]; thereby suggesting an enhanced therapeutic potential for CCNG1/Cyclin G1 oncogene as a molecular-genetic marker and a postulated target for treating colorectal neoplasias.
In 2012, Russell et al. [36] reported that Cyclin G1 regulates the outcome of taxane-induced mitotic checkpoint arrest demonstrating that CCNG1 amplification promotes “cell survival” after paclitaxel exposure in ovarian cancer cells. Conversely, CCNG1 depletion by RNA interference enhanced paclitaxel-induced cell death via apoptosis. Further, CCNG1 amplification was associated with significantly shorter post-surgical survival in patients with ovarian cancer who had received adjuvant chemotherapy with taxanes and platinum compounds [36]. Indeed, CCNG1 overexpression per se was determined to promote epithelial-mesenchymal transition (EMT) to an aggressive “metastatic” phenotype, which is mechanistically associated with chemotherapy resistance in gastric, liver, ovarian and other cancer types [8-10, 37].
The mechanisms of oncogene addiction and cancer progression include loss of natural tumor suppression focused on CCNG1/Cyclin G1 proto-oncogene: in 2007, a series of high-throughput screens investigating the role of microRNAs in human hepatocellular carcinoma (HCC) identified miR-122 as the leading species of microRNA that was either lost or significantly down-regulated in about 70% of HCCs, and in all of the HCC cell lines [38]. Notably, these studies demonstrated CCNG1as a gene target of miR-122, due to the inverse relationship between miR-122 and CCNG1 expression seen in HCC. Loss of miR-122 gene suppression and consequential CCNG1 overexpression was associated with increased proliferation of HCC cells, disease progression, and metastasis [39], while re-expression of miR-122 was shown to inhibit both their tumorigenic properties [40] and metastatic potential [9,41]. It was confirmed that, by controlling CCNG1 expression, miR-122 impacted the stability and transcriptional activity of p53, as restored miR-122 expression reduces the metastatic invasiveness of HCC-derived cell lines [41]. Moreover, the inhibitory effect of experimentally restored miR-122 expression on CCNG1 levels increased the sensitivity of HCC cells to both sorafenib [40] and doxorubicin [41], thereby establishing a mechanistic basis for the future development of combined chemotherapy and miR-122 mimetic and/or CCNG1-based cancer therapies.
This is the first study that uses bioinformatics and a qualified IHC protocol to study a large number of tumors for CCNG1 expression compared to their analogous counterparts. As cancer treatment continues to trend toward more highly directed molecular therapies, efforts have been made to determine how to best assess which patients may benefit from specific targeted therapies. Cyclin G1 dysregulation is an important negative regulator of p53 activity, allowing for disinhibited cell cycle progression with decreasing DNA fidelity [3,4]. In the present study, we found that Cyclin G1 is overexpressed in many tumor samples; and that in metastatic tumors, Cyclin G1 expression is higher than that of the Ki-67 labeling index of cell proliferation (an important prognostic factor), providing mechanistic support for a Cyclin G1-centric view of cancer stem cell Competence, as distinguishable, in terms of aligning targets with prospective therapies, from the enzymatic and biochemical phases of proliferative cell cycle control. Together with the broad clinical efficacy of CCNG/Cyclin G1 inhibitor (DeltaRex-G) therapy, this finding supports the emerging focus on the Cyclin G1 oncogene [3,4], which should be included in the molecular-genetic profiling of tumors at diagnosis and in post-treatment tumor specimens.
DeltaRex-G is the first and, so far, only tumor-targeted retrovector encoding a CCNG1 inhibitor gene [15-22], expressed therapeutically as a gene-edited dominant-negative (dnG1), i.e., a cytotoxic Cyclin G1 pathway-blocking construct [3,4]. DeltaRex-G has been found to be of significant and durable clinical benefit in an array of advanced metastatic cancers, as salvage therapy [19-25]; therefore, the ability to screen and identify patients with specific overexpression of the commanding CCNG1 proto-oncogene can help inform clinicians as to which patients might benefit the most from CCNG1 inhibitor therapy. Additionally, finding that CCNG1 expression varied over time in some tumors suggests that genomic data from multiple biopsies or from circulating cell-free tumor DNA may be additionally informative, in relation to predicting the optimal timing and duration of DeltaRex-G and other future CCNG1 gene-based cancer therapies.
Our findings in clinical tumors—that Cyclin G1 is over expressed in tumor cells at metastatic sites when compared to primary tumors—is in agreement with clinicopathological analysis in HCC [9], wherein the pivotal role of CCNG1/Cyclin G1 expression in cancer progression is viewed as a novel prognostic biomarker and prospective therapeutic target for the clinical management of metastatic disease. One important pathway driving the epithelial-mesenchymal transition (EMT) of metastatic cancers is the stabilization of the “Snail-family” of transcription factors, described as a molecular EMT “switch” to a motile and aggressive phenotype characterized by increased invasive potential, cytoskeletal reorganization, and molecular-genetic down regulation of E-cadherin [9,42], required for maintenance of epithelial architecture. Biochemically, GSK-3β kinase phosphorylates Snail, a transcriptional repressor involved in negative regulation of E-cadherin and a marker of malignancy [43,44]. Conceptually, the Cyclin G1 Axis promotes EMT and cancer metastasis, in part, via activation of the PI3K/Akt/ GSK-3β/Snail-dependent pathway, suggesting that two parameters: Akt-activation in correlation with elevated Cyclin G1 levels may be a more powerful predictor of a poor prognosis [9,45].
This study also found CCNG1/Cyclin G1 to be overexpressed, not just in flagrant tumor cells, but within the supportive neovascular and stromal cells of the tumor microenvironment (TME) as well. The term “angiogenic switch” describes the point in tumor progression when pro-angiogenic factors begin to predominate over anti-angiogenic factors, leading to vascular proliferation in the TME, allowing the tumor to receive nutrients required to progress and to maintain its high energy demand [46,47]. Additionally, TME vasculature encourages evasion of antitumor immune surveillance, in part by impeding lymphocyte-endothelial cell interaction and upregulating immunosuppressive leukocytes [11,47]. The specific cytocidal activity of DeltaRex-G in human tumors, including proliferative tumor-associated TAMs and TAFs suggests that DeltaRex-G breaks anergy by enhancing immune cell trafficking within the TME [24]. Moreover, localized GMCSF-immune stimulation, in combination with Cyclin G1 blockade, has demonstrated promising clinical results and survival value in advanced metastatic cancers [21], while chemo-sensitization, has been experimentally demonstrated in the medical literature [40,41]. Taken together with the notable therapeutic efficacy and long-term survival milestones achieved in advanced cancers with tumor-targeted dnG1 (DeltaRex-G) [3-4,22-23,48], the pivotal and commanding role of the CCNG1 oncogene (Cyclin G1/Cdk/Myc/Mdm2/p53 Axis) of cancer stem cell Competence provides a unifying perspective for advancing new combinatorial and molecular approaches to cancer management [4,24,48-50]. Phase 2/3 studies are planned to identify patients who are likely to respond favorably and/or benefit most with DeltaRex-G gene therapy by correlating CCNG1 expression levels and treatment outcome parameters in cancer patients treated with DeltaRex-G with or without chemotherapy, targeted therapy and/or immunotherapy, revealed in the profile of oncogene expression.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
